Search for topics or resources
Enter your search below and hit enter or click the search icon.
With a full suite of fertility services, award-winning labs, holistic support offerings, and a unique approach to the patient experience, you'll receive comprehensive care from start to finish.


Experience personalized care with tailored treatment plans, a unique team approach and our multidisciplinary Integrated Fertility & Wellness program.

Our above-average success rates mean that achieving your fertility and family-building goals may be a lot closer than you think.

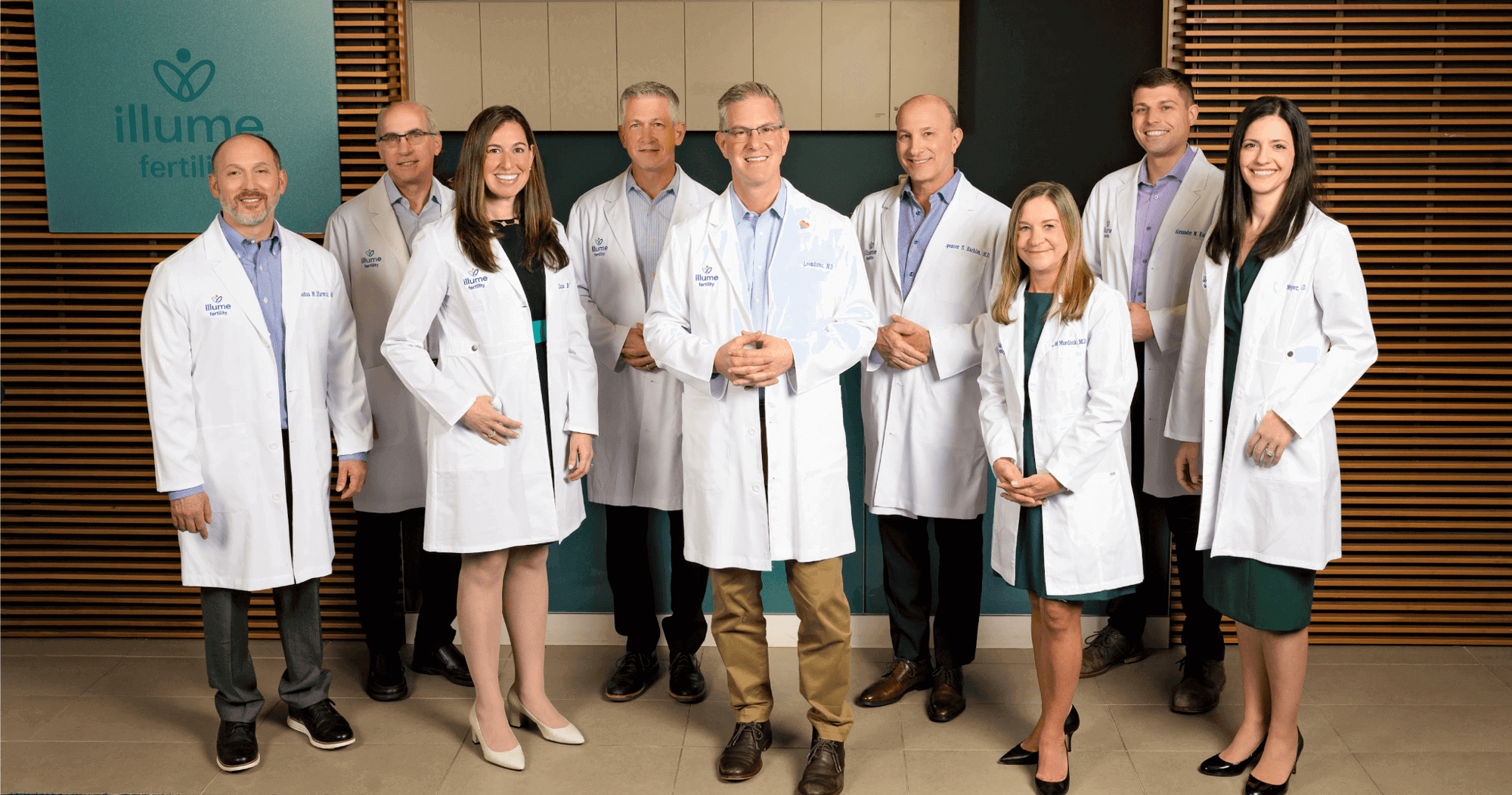
Receive expert guidance from our award-winning team of nine board-certified reproductive endocrinologists, whose only goal is your success.
Not being able to grow your family in the way you anticipated can be overwhelming and frustrating. If you’re tired of feeling stuck and ready to start making real progress towards your family-building goals, Illume Fertility is here to help.

Get the care you deserve with the help of Illume Fertility’s team of expert medical and wellness professionals, all dedicated to supporting you throughout your journey.

After you contact us, one of our New Patient Liaisons will reach out within 48 hours to set up your first consult and help you get started.
This vital step of the process uncovers root causes of infertility and offers insight on what you need to get to where you want to be.
With answers in hand, you and your Care Team will plot the path to success and work together to achieve your goals.



We know that you’re eager to grow your family and may not have envisioned needing support to make those dreams come true. That’s why we're so passionate about providing you with the highest level of care to help you achieve your goals. We’re ready to help you feel more confident and in control of your reproductive health.

.png?width=150&height=150&name=Logo%20slider%20homepage%20Illume%20(1).png)
.png?width=150&height=150&name=Logo%20slider%20homepage%20Illume%20(2).png)











Learn how our expert team can help you prepare for next steps and achieve your fertility goals. Schedule your consult today.